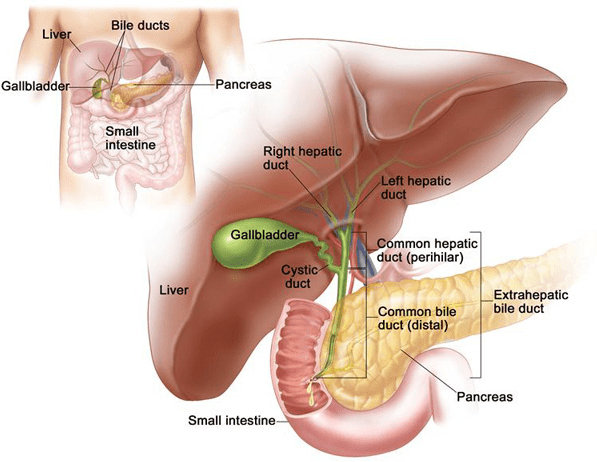

Gallstones & Cholecystitis
Hardened cholesterol or pigment deposits that form inside the gallbladder. When stones block the exit channel (cystic duct), it causes severe episodic pain (biliary colic); prolonged blockages lead to acute or chronic gallbladder inflammation (cholecystitis) and localized infections.
Biliary Obstruction & Choledocholithiasis
A condition where gallstones migrate out of the gallbladder and become trapped inside the main structural channel (the common bile duct). This blocks the continuous flow of bile from the liver, leading to obstructive jaundice, dark urine, pale stools, and potential liver cell irritation.
Cholangitis
A severe, rapid bacterial infection of the bile ducts caused by a persistent blockage. It is a clinical emergency characterized by a combination of high fever with chills, right-sided abdominal pain, and deep jaundice, requiring immediate clearing of the obstruction.
Benign Bile Duct Strictures
A physical narrowing of the bile duct lumen, usually resulting from scar tissue formation after previous abdominal surgeries, chronic inflammation, or deep biliary tract infections. It gradually restricts fluid movement and requires mechanical widening or surgical reconstruction.
Gallbladder Cancer
A malignancy originating within the mucosal lining of the gallbladder. Early stages are often discovered incidentally after routine stone removals, while advanced stages require extended surgical clearance that includes removing adjacent liver tissue and local lymph nodes.